- +91 9848014512
- +91 9951414512


Standard medical textbooks define infertility as the “failure to conceive following one year of unprotected sexual intercourse.” For young and healthy heterosexual couples having frequent intercourse, about 85% will be pregnant after one year of trying and about 93% will be pregnant after two years of trying to conceive.
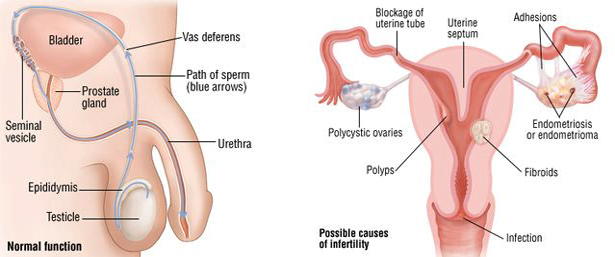
Failure to conceive following one year of unprotected intercourse if under 35 years of age or six months if over 35.
Initial infertility evaluations should be individualized by an infertility specialist, taking into consideration the medical history of the couple and the age of the female partner.
It is important to understand that human reproduction appears to be relatively inefficient. In any one month, it is estimated that of 100 young and healthy heterosexual couples attempting to conceive, about 25 couples will successfully do so and about 75 will fail. True infertility only occurs in a few specific situations:
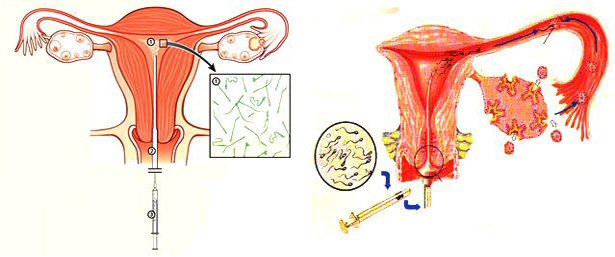
Intrauterine insemination (IUI) is a relatively low tech assisted conception service (fertility treatment). Intrauterine insemination involves preparing the male partners sperm in the laboratory and then placing only those sperm which move well and are normally formed in the women’s uterus. The sperm are transferred into the uterus at the time of ovulation. IUI can be performed with the sperm of the male partner or with donor sperm.
The success of intrauterine insemination depends on 2 factors:
In general intrauterine insemination is a good assisted conception treatment if it is performed to overcome a problem of lack of sperm ie using donor sperm for severe male subfertility, and for single women or lesbian couples. It is also successful if intercourse is not occurring normally such as in cases of ejaculation dysfunction (ED). Intrauterine insemination is moderately successful when used for cervical mucus hostility when sperm are killed within the cervix. Intrauterine insemination tends to be less useful if the indication is male factor subfertility ie low numbers or movement of sperm or in unexplained infertility.
For women who are not ovulating regularly, the goal of treatment is to mature and ovulate a single egg – ovulation induction (OI) as referred to previously. Clomiphene alone often works well to cause the ovaries to mature an egg. A typical protocol will involve taking clomiphene each day for cycle days 3-7 or cycle days 5-9. Ultrasounds and blood tests are then used to monitor the egg as it matures. Once the egg is ready, a subcutaneous injection is given of a hormone called hCG (the ‘trigger shot’), which triggers ovulation of that egg approximately 38-40 hours after the injection.
In women whose irregular ovulation is due to PCOS, a medication called metformin may be added to the treatment regimen. For those women who do not respond to clomiphene, FSH may be added to the protocol. In women who do not ovulate due to hypothalamic amenorrhea, injectible medications containing both FSH and LH are used to stimulate the ovaries to mature an egg. An Intrauterine Insemination (IUI) is commonly performed in the OI cycle.
Intrauterine insemination (IUI) is a relatively low tech assisted conception service (fertility treatment). Intrauterine insemination involves preparing the male partners sperm in the laboratory and then placing only those sperm which move well and are normally formed in the women’s uterus. The sperm are transferred into the uterus at the time of ovulation. IUI can be performed with the sperm of the male partner or with donor sperm.
The success of intrauterine insemination depends on 2 factors:
In general intrauterine insemination is a good assisted conception treatment if it is performed to overcome a problem of lack of sperm ie using donor sperm for severe male subfertility, and for single women or lesbian couples. It is also successful if intercourse is not occurring normally such as in cases of ejaculation dysfunction (ED). Intrauterine insemination is moderately successful when used for cervical mucus hostility when sperm are killed within the cervix. Intrauterine insemination tends to be less useful if the indication is male factor subfertility ie low numbers or movement of sperm or in unexplained infertility.
For women who are not ovulating regularly, the goal of treatment is to mature and ovulate a single egg – ovulation induction (OI) as referred to previously. Clomiphene alone often works well to cause the ovaries to mature an egg. A typical protocol will involve taking clomiphene each day for cycle days 3-7 or cycle days 5-9. Ultrasounds and blood tests are then used to monitor the egg as it matures. Once the egg is ready, a subcutaneous injection is given of a hormone called hCG (the ‘trigger shot’), which triggers ovulation of that egg approximately 38-40 hours after the injection.
In women whose irregular ovulation is due to PCOS, a medication called metformin may be added to the treatment regimen. For those women who do not respond to clomiphene, FSH may be added to the protocol. In women who do not ovulate due to hypothalamic amenorrhea, injectible medications containing both FSH and LH are used to stimulate the ovaries to mature an egg. An Intrauterine Insemination (IUI) is commonly performed in the OI cycle.
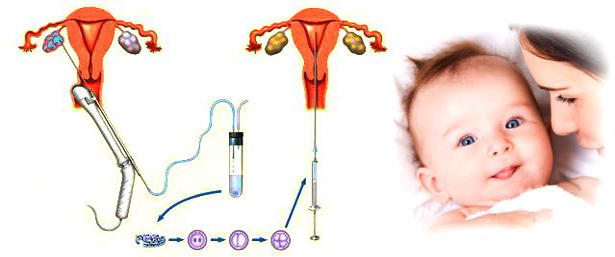
ICSI is a highly advanced type of in vitro fertilisation (IVF) treatment where fertilisation is achieved after injecting a single sperm into each egg of the female partner. With the benefit of ICSI we are able to obtain fertilisation when very few sperms are obtained from men who are sterile due to the problems above. Sperms are taken by the minimally invasive techniques, usually under local anaesthetic. The man can leave the Clinic shortly afterwards to accompany his partner who will be having her egg collection at the same time.
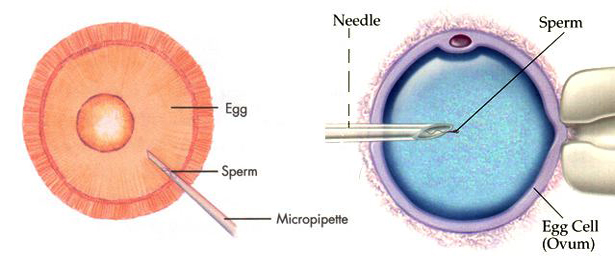
ICSI is a refinement of the traditional IVF procedure. Eggs and sperm are collected in exactly the same way as in IVF, but instead of the sperm being mixed with the egg, one single sperm of the best quality is selected, , and this is then injected directly into the egg to achieve fertilisation. The procedure then follows usual IVF, with the resulting embryo transferred to your uterus to continue growing as in normal pregnancy.
ICSI is used when the fertility problem is a result of sperm disorders. These can include a low sperm count, poor quality sperm or poor sperm motility or the presence of antisperm antibodies. It gives hope to people who have a sperm problem, but who want to use their own sperm to conceive a child. ICSI is recommended for patients who have had previously had failed fertilisation with IVF or a very poor number fertilised. It is also necessary for surgically-retrieved sperm.
ICSI is offered by many infertility clinics. At Manchester Fertility Services, ICSI is only used where the cause of the infertility has been identified as lying with the male partner and when conventional IVF has failed. There is no reason to use ICSI where the male partner does not have any sperm disorders or where the cause is with the female partner. In these instances, traditional IVF should always be the first option.
Yes. Be wary of a clinic which performs high rates of ICSI procedures. It could indicate that their conventional IVF results are poor. Here at Manchester Fertility Services, ICSI is only used where absolutely necessary.
At Padmaja Fertility Services, we offer sperm freezing. It is simply a way of preserving a sample of your sperm until you wish to try for a family.
There are many reasons why men freeze their sperm. Most common are:
Freezing sperm is a simple process. Before you freeze your sperm you will undergo screening to make sure you’re free of any infectious diseases. You will also be offered the opportunity to discuss the implications of sperm freezing with one of our experienced counsellors.

You will need to give written consent for your sperm to be used. The consent form allows you to specify what happens to your sperm in the event that something happens to you and how long you want your sperm sample to be preserved for. You can withdraw your consent for the use of your sperm at any time.
You then visit our clinic and provide a fresh sperm sample, which is then preserved in liquid nitrogen.
When you decide you wish to use your sperm, it is thawed and analysed by our team of andrologists to make sure it is of good enough quality to be used.
The chances of pregnancy using frozen sperm depends on a number of factors. These include how successfully your sperm survives the freeze-thaw process. Your sperm can be used in IVF or ICSI treatment.
Cryopreservation of semen involves the cooling of a sperm and storage at a temperatureВ where all metabolic processes are arrested. In practice, frozen sperms are stored at the temp. of -196°C in liquid nitrogen.
Egg donation has been a standard form of fertility treatment since 1984. It is used in women in whom the ovaries have lost the ability to produce eggs of a suitable quality, or in some cases have lost the ability to produce eggs at all, e.g. premature ovarian failure. In these circumstances there is nothing wrong with the uterus itself and patients can successfully become pregnant using donated eggs with no increased risk to the pregnancy. In fact, in egg donation the chance of pregnancy is higher than in normal IVF treatment mainly because donors tend to be younger and more fertile than women seekingIVF treatment with their own eggs.
Our team has been very active in our attempts to raise awareness of the need for egg donors over recent years and we are very conscious of the enormous gift that donors are making to an infertile couple. Egg donation at our Clinic is usually anonymous but we will accept known donors (following careful consideration on a case by case basis) providing they fall within the criteria discussed in the paragraph egg donors

All sperm donors at IVFAustralia must adhere to practices developed by the Reproductive Technology Accreditation Committee of the Fertility Society of Australia, and the National Health and Medical Research Council, including:
The first step is a consultation with a fertility specialist, followed by a semen analysis and compulsory counselling. We discuss legal, social, genetic and moral implications of the donation as well as the health checks and procedures involved.
Sperm donors need to be prepared to discuss and provide the following types of information: